Prevention, Early Detection And Treatment Of Acute And Chronic Complications Of Diabetes.
Diabetes is a silent killer, which kills part by part of our life.
According to International Diabetes Federation (IDF), the number of people with diabetes worldwide is projected to increase from 382 million in 2013 to 592 million by 2035 (Journal Endocrinology, 2015).
At present In India we have 65 million DIABETES and 77 million in PRE-DIABETES ZONE. Diabetes is an increasing health burden in India. India is the diabetes capital of the world. It is widely accepted fact that 35 – 40% of people show presence of diabetes related complications at the time of diagnosis.
The Complications of Diabetes mellitus are far less common and less severe in people who have well controlled blood sugar levels.
Acute complications include hypoglycemia(refer to Hypoglycemia) and hyperglycemia(refer to Hyperglycemia), diabetic coma and nonketotic hyperosmolar coma.
It causes many diseases related to the heart, cholesterol, nerves, feet, eyes and circulatory system if uncontrolled for a long time. Since PREVENTION IS BETTER THAN CURE, a multi-displinary approach is required to control the disease and more important to prevent complications.
Every patient is unique hence the diabetes clinic offers comprehensive medical care for diabetic patients based on their unique requirements. The diabetes clinic offers following services.
Cardiovascular
As CVD is the leading cause of morbidity and mortality for individuals with diabetes and is the largest contributor to the direct and indirect costs of diabetes.
In all patients with diabetes, cardiovascular risk factors should be systematically assessed at least annually.
Risk factors include:

- Hypertension
- Dyslipidaemia
- Smoking
- Family History of Premature Coronary Disease &
- Albuminuria.
Management
- Measuring Blood pressure at every routine visit.
- Targeting Blood pressure for patients with diabetes and hypertension and other disorders.
- Annual ECG evaluation to rule out ischemic heart disease.
- Optimizing glycaemic control for patients by using suitable medications.
- Optimizing elevated lipid profile through intensive lifestyle therapy and medications.
- Encouraging a lifestyle intervention consists of change in dietary pattern & weight loss – if overweight or obese and increased physical activity.
- Screening diabetes distress using validated and appropriate measures & psychosocial problems and other barriers to diabetes self-management such as limited financial, logistical, and support resources.
- Referring to a cardiologist if required.

Retinopathy
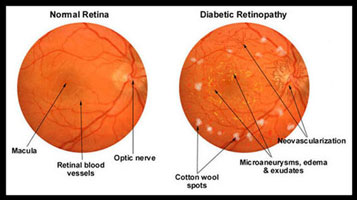
Diabetic retinopathy is the most common preventable cause of blindness in diabetic patients.
Frequent high blood sugars in diabetics are associated with damage to the tiny blood vessels in the retina, leading to diabetic retinopathy.
Retina detects light and converts it to signals sent through the optic nerve to the brain.
Diabetic retinopathy can cause blood vessels in the retina to leak fluid or haemorrhage, distorting the vision.
In its most advanced stage, new abnormal blood vessels proliferate on the surface of the retina, which can lead to scarring and cell loss in the retina.


Signs and Symptoms:
- Seeing spots or floaters
- Blurred vision
- Having a dark or empty spot in the centre of the vision
- Difficulty in seeing well especially at night.
Management
- Optimize glycaemic control to reduce the risk or slow the progression of diabetic retinopathy.
- Optimize blood pressure and serum lipid control to reduce the risk or slow the progression of diabetic retinopathy.
- Annual eye examination by an ophthalmologist/ Referral ophthalmologist.
Nephropathy
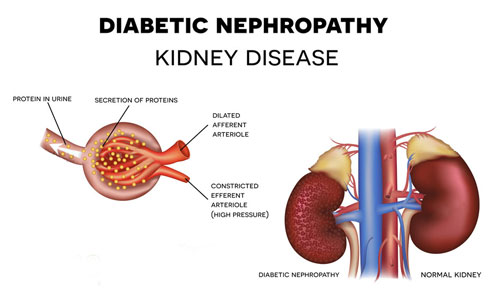
Diabetic Nephropathy (DN), also known as Diabetic Kidney Disease (DKD) is one of the most important long-term complications of diabetes and the most common cause of end-stage renal disease (ESRD) worldwide. DKD occurs in type 1 & type 2 diabetes mellitus and other secondary forms of diabetes and is defined as structural and functional renal damage manifested as clinically detected albuminuria in the presence of normal or abnormal glomerular filtration rate (GFR).
DKD develops after the initial 10-15 years of disease onset in type 1 diabetes, whereas the onset is not clearly defined in type 2 due to the late diagnosis of diabetes in some patients.
Screening and Diagnosis of Diabetic Nephropathy:
- Screened annually with S. Creatinine and eGFR and Urine Alb:Creat (ACR)
Starting 5 years after diagnosis of type 1 diabetes & starting at the diagnosis of type 2 diabetes - Elevated Urine ACR confirmed > 2 times and not in setting of UIT (Urinary tract infections), acute febrile illness, vigorous exercise, uncontrolled hypertension and heart failure.
Microalbuminuria: ACR – 3 to 30 mg/ mmol
Macroalbuminuria: ACR – >300 mg/ mmol
Signs and Symptoms:
- Pedal oedema
- Nausea & vomiting
- Decreased urine
- Inching skin
The treatment goals for Diabetic Kidney Disease (DKD) are to manage glycaemic control, maintain blood pressure and lipid profile, to prevent further cardiovascular events & slow the progression of the renal disease.
Management

- Assessing urinary Albumin: Creatinine ratio with Afinion Analyser in patients with Type 1 & Type 2 diabetes
- Setting and reaching blood pressure goal
- Optimizing glucose control to reduce the risk or slow the progression of diabetic kidney disease.
- Provide nutrition support by developing or maintaining healthy lifestyle habits, which help to maintain Blood pressure and blood glucose levels.
- Screening diabetes distress using validated and appropriate measures & psychosocial problems and other barriers to diabetes self-management such as limited financial, logistical, and support resources.
Neuropathy
Peripheral neuropathy, a result of damage to your peripheral nerves, often causes weakness, numbness and pain, usually in your hands and feet. It can also affect other areas of your body.
Management
- All patients should have annual 10-g monofilament testing to identify feet at risk of ulceration and amputation.
- Assessment for diabetic peripheral neuropathy (DPN) starting at diagnosis of type 2 diabetes and 5 years after the diagnosis of type 1 diabetes and at least annually thereafter.
- Evaluation for distal symmetric polyneuropathy should include a careful history and assessment of either temperature or pinprick sensation (for small-fiber function) and vibration sensation using a 128-Hz tuning fork (for large-fiber function).
- Optimize glucose control to prevent or delay the development of neuropathy in patients with type 1 diabetes and to slow the progression of neuropathy in patients with type 2 diabetes.